NEEL RAYA MD INC.
HISTORY
·
CHIEF COMPLAINT
·
HISTORY OF PRESENTING ILLNESS
Symptom
- OPQRST
O: Onset-how
did it start, duration of symptom, frequency of the symptom
P:
Provocation/Position or location
What brought symptoms on?, Where is pain located?
Q:
Quality
Sharp, dull, crushing, colic and so on.
R:
Radiation
Does pain travel?
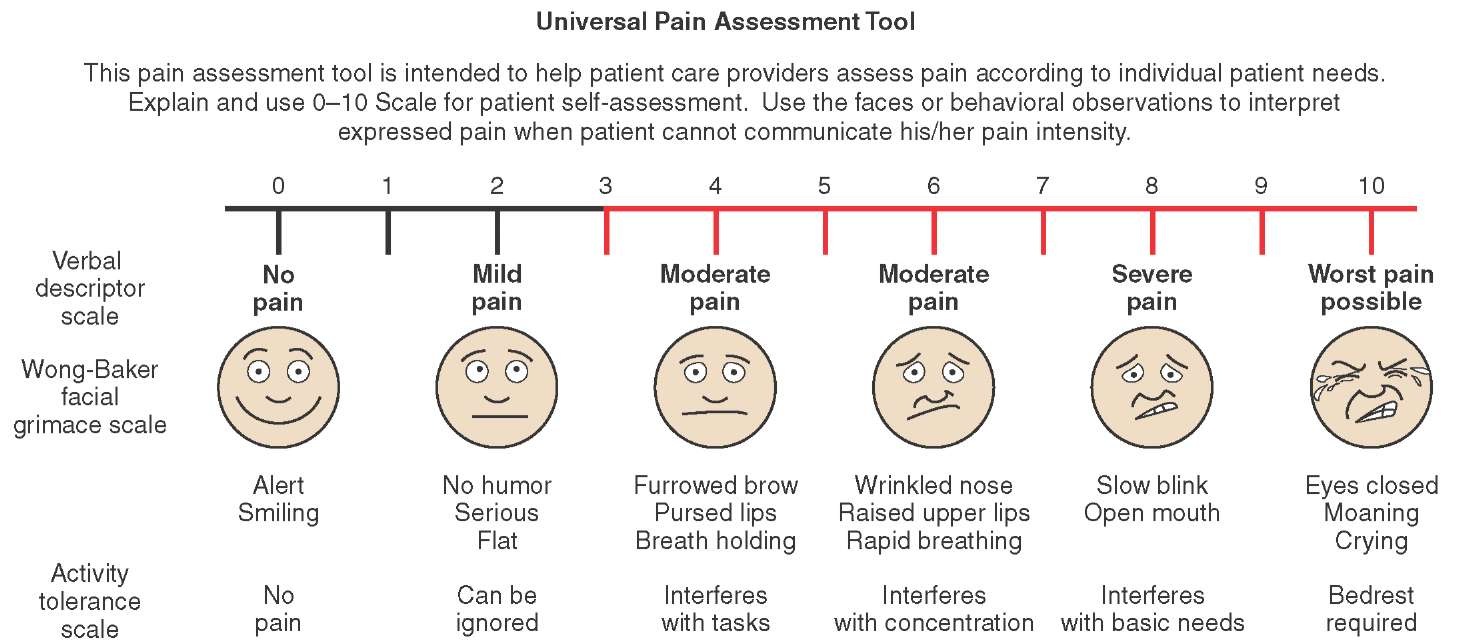
S: Severity/Symptoms
Associated
1/10 scale, What other symptoms occur?
T:
Timing/Triggers
Occasional, constant, intermittent, only with
certain activities, what brings symptoms, what relieves symptoms,
example-activity, movement, eating, breathing.
Also
check
·
functional
impairment – example new York heart association for CHF congestive heart
failure.
·
patient's
interpretation of symptom – what does patient make of the illness – gives
insight.
How to approach Patient Symptoms
·
Identify
accurately the symptom that patient is describing.
·
Anatomical
diagnosis - think of which anatomical organs can produce the symptoms – use the
list from Isabel - ask appropriate questions.
·
Pathological
diagnosis – question patient based on possible conditions.
·
Etiological
diagnosis – from other elements of history – Social, Family, Medications, and
others
·
Differential
diagnosis – make a list – at end of clinical history, before starting Physical
exam.
Reference - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4345897/
The remainder of
the history is obtained after completing the HPI. As such, the previously
discussed techniques for facilitating the exchange of information still apply.
Past Medical History: Start
by asking the patient if they have any medical problems. If you receive little/no
response, the following questions can help uncover important past events: Have
they ever received medical care? If so, what problems/issues were addressed?
Was the care continuous (i.e. provided on a regular basis by a single person)
or episodic? Have they ever undergone any procedures, X-Rays, CAT scans, MRIs
or other special testing? Ever been hospitalized? If so, for what? It's quite
amazing how many patients forget what would seem to be important medical
events. You will all encounter the patient who reports little past history
during your interview yet reveals a complex series of illnesses to your
resident or attending! These patients are generally not purposefully concealing
information. They simply need to be prompted by the right questions!
Past
Surgical History: Were they ever
operated on, even as a child? What year did this occur? Were there any
complications? If they don't know the name of the operation, try to at least
determine why it was performed. Encourage them to be as specific as possible.
Medications: Do they take any prescription medicines? If so, what is the
dose and frequency? Do they know why they are being treated?* Medication
non-compliance/confusion is a major clinical problem, particularly when
regimens are complex, patients older, cognitively impaired or simply
disinterested. It's important to ascertain if they are actually taking the
medication as prescribed. This can provide critical information as frequently
what appears to be a failure to respond to a particular therapy is actually
non-compliance with a prescribed regimen. Identifying these situations requires
some tact, as you'd like to encourage honesty without sounding accusatory. It
helps to clearly explain that without this information your ability to assess
treatment efficacy and make therapeutic adjustments becomes
difficult/potentially dangerous. If patients are, in fact, missing doses or not
taking medications altogether, ask them why this is happening. Perhaps there is
an important side effect that they are experiencing, a reasonable fear that can
be addressed, or a more acceptable substitute regimen which might be
implemented. Don't forget to ask about over the counter or
"non-traditional" medications. How much are they taking and what are
they treating? Has it been effective? Are these medicines being prescribed by a
practitioner? Self administered?
* You'll
be surprised to learn how many patients don't know the answers to these
questions. Encourage them to keep an up to date medication list and/or write
one out for them. When all else fails, ask the patient to bring their meds with
them when they return or, if they are in-patients, see if a family
member/friend can do so for them.
Allergies/Reactions: Have they experienced any adverse reactions to medications?
The exact nature of the reaction should be clearly identified as it can have
important clinical implications. Anaphylaxis, for example, is a life
threatening reaction and an absolute contraindication to re-exposure to the
drug. A rash, however, does not raise the same level of concern, particularly
if the agent in question is clearly the treatment of choice.
Smoking
History: Have they ever smoked
cigarettes? If so, how many packs per day and for how many years? If they quit,
when did this occur? The packs per day multiplied by the number of years gives
the pack-years, a widely accepted method for smoking quantification. Pipe,
cigar and chewing tobacco use should also be noted.
Alcohol: Do they drink alcohol? If so, how much per day and what type
of drink? Encourage them to be as specific as possible. One drink may mean a
beer or a 12 oz glass of whiskey, each with different implications. If they
don't drink on a daily basis, how much do they consume over a week or month?
Other
Drug Use: Any drug use, past or
present, should be noted. Get in the habit of asking all your patients these
questions as it can be surprisingly difficult to accurately determine who is at
risk strictly on the basis of appearance. Remind them that these questions are
not meant to judge but rather to assist you in identifying risk factors for
particular illnesses (e.g. HIV, hepatitis). In some cases, however, a patient
will clearly indicate that they do not wish to discuss these issues. Respect
their right to privacy and move on. Perhaps they will be more forthcoming at a
later date.
Obstetric
(where appropriate): Have they ever been
pregnant? If so, how many times? What was the outcome of each pregnancy (e.g.
full term delivery; spontaneous abortion; therapeutic abortion).
Sexual
Activity: This is an uncomfortable line
of questioning for many practitioners. However, it can provide important
information and should be pursued. As with questions about substance abuse,
your ability to determine on sight who is sexually active (and in what type of
activity) is rather limited. By asking all of your patients these questions,
the process will become less awkward. Do they participate in intercourse? With
persons of the same or opposite sex? Are they involved in a stable
relationship? Do they use condoms or other means of birth control? Married?
Health of spouse? Divorced? Past sexually transmitted diseases? Do they have
children? If so, are they healthy? Do they live with the patient?
Family
History: In particular, you are
searching for heritable illnesses among first or second degree relatives. Most
common, at least in America, are coronary artery disease, diabetes and certain
malignancies. Patients should be as specific as possible. "Heart
disease," for example, includes valvular disorders, coronary artery disease
and congenital abnormalities, of which only coronary disease has genetic
implications. Find out the age of onset of the illnesses, as this has
prognostic importance for the patient. For example, a father who had an MI at
age 70 is not a marker of genetic predisposition while one who had a similar
event at age 40 certainly would be. Also ask about any unusual illnesses among
relatives, perhaps revealing evidence for rare genetic conditions.
Work/Hobbies/Other: What sort of work does the patient do? Have they always done
the same thing? Do they enjoy it? If retired, what do they do to stay busy? Any
hobbies? Participation in sports or other physical activity? Where are they
from originally? These questions do not necessarily reveal information directly
related to the patient's health. However, it is nice to know something
non-medical about them. This may help improve the patient-physician bond and
relay the sense that you care about them as a person. It also gives you
something to refer back to during later visits, letting the patient know that
you paid attention and really remember them.
Military
Service: For obvious reasons, serving
in the armed forces can be an important period in someone's life. In addition,
inquiring about physical trauma, mental health issues (PTSD, depression,
substance abuse), and unusual exposures (toxins, infections) may reveal
important information.
In recounting their history, patient's frequently drop clues that suggest
issues meriting further exploration. If, for example, they are taking
anti-hypertensive or anti-anginal medications yet made no mention of cardiac
disease, additional history taking would be in order. Furthermore, if at any
time you uncover information relevant to the chief complaint don't be afraid to
revisit the HPI.
PHYSICAL
EXAM
·
PULSE
·
BLOOD
PRESSURE
·
RESP RATE
·
TEMP
·
WEIGHT
·
SHOULDER
EXAM
·
SPECIAL-TESTING
speed
test, empty can test, slap test, neer’s
test, Hawkins test, drop-arm test, belly press test, lift-off test, jobe test, apprehension test-anterior
instability, anterior instability,
posterior apprehension, jerk sign, sulcus sign.
·
KNEE EXAM
·
Tests of knee ligaments and menisci
·
BACK EXAM
·
Inspection, Palpation, tests -
https://www.youtube.com/watch?v=5_txE56X2-8&feature=youtu.be
·
CARDIOVASCEXAM
·
Inspection, Palpation,
tests
·
RESPIRATORY
EXAM
·
NEUROLOGICAL
EXAM
·
ABDOMINAL EXAM
– GI & RENAL
TESTS
·
EKG - procedure
·
VISUAL
SCREEN - testing
{kind=link}